


How to Write SOAP Notes for Physical Therapy (With Real Examples)


After reviewing hundreds of physical therapy SOAP notes, I’ve seen that most fail because they lack clarity, not detail. If you’re wondering how to write SOAP notes for physical therapy that are clear and defensible, I’ll walk you through the format using real examples.
How to write SOAP notes for physical therapy
To write SOAP notes for physical therapy, you document patient reports, objective measurements, clinical reasoning, and treatment plans using a clear four-part format.
Subjective (S)
This section records what the patient tells you. Write down their complaints, how they describe pain, and what activities they can't do.
Here's what to include:
- Pain details: Where does it hurt? How bad is it on a 0-10 scale? Is it sharp or dull? When does it hurt most?
- What they can't do: Real activities matter more than general complaints. "I can't lift my arm to wash my hair" tells you more than "shoulder hurts."
- How they think they're doing: Do they feel better, worse, or the same since last visit?
- Exact quotes: Use their words. Put quotation marks around key phrases. "The pain is a 7/10 when I stand up" is better than paraphrasing.
Keep this section focused. You don't need their full history every time. Just write what's relevant today.
Objective (O)
This section is for measurements and what you observe. Write down what you see, test, and measure during the session.
Include these parts:
- Numbers: Range of motion in degrees. Strength grades (0-5 scale). Test results. Outcome measures. Numbers matter here.
- What you see: Posture. How they walk. Swelling. Muscle guarding. Any movements that look off.
- What you feel: Tenderness when you touch muscles. Tight muscles. Trigger points. Temperature changes.
- Test results: Did special tests come back positive or negative? Balance test scores. Any standardized measures.
Be specific. "Right knee flexion 85°" is better than "limited knee flexion." Anyone reading your note should picture what you saw.
Assessment (A)
This is where you interpret the subjective and objective findings and explain what they mean clinically. The assessment should clearly connect measurable changes to functional goals and justify continued skilled treatment.
Cover these points:
- Goal progress: Document whether the patient is improving, plateauing, or regressing. Reference specific functional goals and measurable changes.
- Treatment response: Describe how the patient responded to today’s session. Note changes in pain levels, range of motion, strength, balance, or functional performance.
- Primary impairments: Identify the key limitations affecting function and connect them directly to activity restrictions.
- Clinical reasoning: Explain why the patient is progressing or not progressing and what that means for the plan of care.
This section demonstrates your clinical judgment. A strong assessment explains why continued treatment is medically necessary and reflects the structured diagnostic reasoning used in physical therapy.
This section shows your skilled judgment. A strong assessment justifies why treatment should continue.
Plan (P)
This section explains what you did today and what happens next. It creates a clear roadmap.
Write down these items:
- Today's treatment: List what you did with details. "Manual therapy to R shoulder, 10 minutes" or "Shoulder exercises: 3 sets of 10 reps with 3 lb weight."
- What you taught: New home exercises. Safety rules you discussed. Self-care strategies.
- Next visit plans: What you'll work on next time. Any tests planned? Treatment changes you want to try.
- Schedule: When they return. Expected treatment length if this is a first visit or progress note.
Your plan should follow from your assessment. If you noted limited shoulder motion in your assessment, your plan should address fixing it.
{{templates}}
Physical therapy SOAP note examples
Physical therapy SOAP note examples include documentation for low back pain, shoulder pain, post-surgical rehab, knee injuries, and balance deficits.
Example 1: Low back pain SOAP note
S: The patient reports low back pain rated 6/10 with sitting and bending forward. “It’s worse after sitting at my desk for more than 30 minutes.” Pain improves with standing and walking, with no symptoms radiating down the legs.
O: Lumbar flexion measures 40° and is limited by pain. Extension is 15° with increased discomfort at the end range. Straight leg raise is negative bilaterally. Paraspinal tightness is noted from L3-L5, and posture shows an increased lumbar curve.
A: Findings support that mechanical low back pain limits sitting tolerance. The patient is progressing toward the goal of tolerating 60 minutes of desk sitting, with pain improving from 8/10 to 6/10 over two visits.
P: Treatment included manual therapy to the lumbar muscles and core stabilization exercises. The patient was educated on workstation setup and scheduled for reassessment in two days.
Example 2: Shoulder pain SOAP note
S: The patient reports right shoulder pain rated 5/10 with overhead reaching and behind-the-back movements. “I can’t reach the top shelf or fasten my bra.” Pain is achy, worse at night, and there was no specific injury.
O: Active shoulder flexion measures 130° with pain at end range, and abduction is 115° with pain above 90°. External rotation is 40°, and internal rotation reaches L3.
A: Strength is 4/5 in the rotator cuff and 5/5 in the deltoid. Hawkins-Kennedy and empty can tests are positive. Posture shows a forward head and rounded shoulders. Findings are consistent with rotator cuff tendinopathy and scapular dyskinesis. The patient is making measurable progress toward the goal of reaching overhead and behind the back without pain, with pain reduced from 7/10 to 5/10.
P: Treatment included manual therapy to the rotator cuff and scapular muscles, followed by shoulder blade stabilization and rotator cuff strengthening exercises. The patient was instructed to continue home exercises daily and return in three days for progression.
Example 3: Knee injury SOAP note
S: The patient reports right knee pain rated 4/10 with stairs and long walks. “Going downstairs is the worst; it feels unstable.” Swelling has decreased since the last visit, and there has been no locking or giving way this week.
O: The right knee measures 38 cm compared to 37 cm on the left, improved from 40 cm at the previous visit. Knee flexion is 120°, with extension lacking 5° of full straightening. Strength is 4/5 in both the quadriceps and hamstrings. Lachman and McMurray tests are negative, and gait shows a slight limp with reduced time on the right side.
A: At four weeks post-ACL repair, findings reflect expected progress. Swelling and range of motion are improving, though quadriceps weakness continues to limit controlled stair descent. The goal remains pain-free, stable stair negotiation.
P: Treatment focused on quadriceps strengthening, straight leg raises, mini squats, heel slides, stair practice, and single-leg balance work. The patient will progress to closed-chain strengthening and additional balance training at the next visit in two days.
Example 4: Post-surgical rehabilitation SOAP note
S: The patient reports left hip pain rated 3/10 at the incision site, improved from 6/10 last week. “I’m walking better, but still need the walker for longer distances.” Sleep has improved, and pain no longer wakes the patient at night.
O: The incision is healing well with no signs of infection. Hip flexion measures 85° within safety limits, abduction 25°, and extension 10°. Strength is 3+ /5 in hip flexors and extensors and 3/5 in abductors. Gait shows reduced hip drop on the left, and transfers are mostly independent with a front-wheeled walker. At three weeks post–total hip replacement, progress is steady.
A: Strength and gait are improving, and the patient remains on track to ambulate household distances without an assistive device, with plans to wean from the walker by weeks five to six.
P: Treatment focused on hip strengthening, walking practice with the walker, and sit-to-stand transfer training. Home exercises were continued, and the next visit will progress to standing hip work and walking tolerance in three days.
Example 5: Balance and gait SOAP note
S: The patient reports feeling unsteady while walking, especially on uneven ground. “I’m afraid I’ll fall when I walk outside.” There was one near-fall at home this week when reaching overhead. The patient uses a single-point cane indoors.
O: The Berg Balance Scale score is 42/56, improved from 38/56 last week, indicating moderate fall risk. Timed Up and Go is 18 seconds with a cane.
A: Gait shows shorter steps, wider stance, reduced arm swing, and a walking speed of 0.7 m/s. Single-leg standing cannot be maintained without support, and balance with eyes closed is limited to 8 seconds. Findings reflect balance deficits with moderate fall risk.
P: Treatment focused on balance training, gait practice over obstacles and at varied speeds, and lower extremity strengthening. A referral to ENT was recommended for further evaluation. The next visit will increase balance challenge and add dynamic walking activities in two days.
SOAP note assessment examples (common patterns)
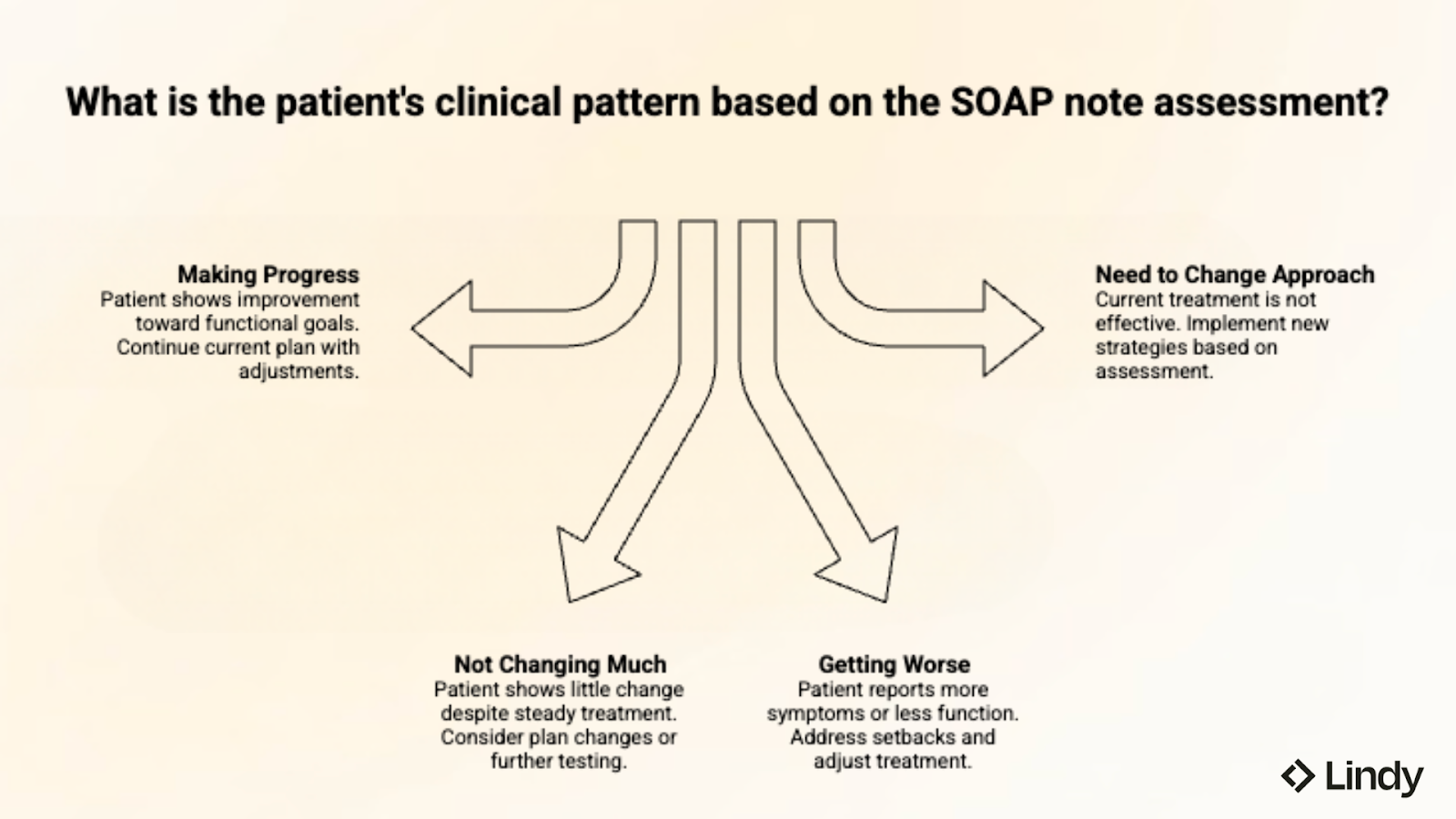
Most SOAP note assessments reflect one of these four clinical patterns:
- Making progress: Patient shows real improvement toward functional goals. Pain decreased. Movement increased. Strength has improved since the last visit. Treatment is working. Continue current plan with changes as needed.
- Not changing much: Patient showing little change over the past 2-3 visits despite steady treatment. May need plan changes, more testing, or referral to another provider. Think about outside factors affecting progress (medication changes, sleep, stress, whether they do home exercises).
- Getting worse: Patient reports more symptoms or less function than on the previous visit. Write down possible causes (doing too much, new injury, illness). Change treatment plan to address setbacks while keeping long-term goals.
- Need to change approach: Current treatment is not producing expected results. Assessment should explain why you're changing and what new strategies you'll try. Connect changes to what you measured and how the patient responded.
Your assessment should always connect to functional goals. "Patient improved shoulder motion by 15°" means more when you add "now able to reach the top cabinet alone."
Common mistakes to avoid
Common SOAP note mistakes include missing measurements, vague Assessments, copied documentation, and Plans that lack treatment detail.
Here’s a short checklist:
- Missing measurements: Writing "movement limited" without recording degrees. Or "strength decreased" without a grade. Always include specific numbers.
- Copying assessment each visit: Pasting "patient progressing toward goals" for five straight visits without showing how or why. Each assessment should reflect that day's findings.
- Vague plans: Ending with "continue current treatment" tells no one what you did or will do. List specific treatments with details and your plan for the next visit.
- Copying full notes forward: Reusing last week’s documentation with only minor edits or a new date. This suggests you’re not reassessing progress or adapting treatment, and raises concerns during insurance reviews.
- Missing the "why": Stating what you measured without explaining what it means clinically. Your assessment should show your thinking, not just repeat measurements.
- Inconsistent terms: Switching between different scales or descriptions across visits makes tracking progress hard. Pick standard terms and stick with them.
{{cta}}
Best practices for physical therapy SOAP notes
Standard rehabilitation texts emphasize measurable outcomes, functional goal tracking, and defensible documentation to support ongoing care (see Physical Rehabilitation, 6th edition).
Here’s what to focus on:
- Document measurable change: Record specific numbers that show progress or decline. For example, knee flexion improved from 95° to 110°, not “patient improved.”
- Connect assessment to measurements: Your assessment should be based on what you measured. If you say the patient is progressing, provide specific measurements that support this claim.
- Keep notes short: Write enough to justify your treatment. Don't bury key information in long paragraphs. Use bullet points and clear sections.
- Show your expertise: Your notes should show why a physical therapist is necessary. Highlight your reasoning, treatment changes based on patient response, and complex problem-solving.
- Update every time: Don't copy last week's notes. Each visit should show what changed, what you saw today, and how your plan changed.
Try Lindy for Automated SOAP Notes
Lindy is an AI assistant that can help handle your SOAP note documentation. After a session, just tell Lindy what happened, and it organizes the details into clear, HIPAA-compliant SOAP notes you can review and sign.
After each visit, Lindy can:
- Match your clinic’s documentation style and terminology
- Capture session details without typing everything manually
- Turn your clinical observations into structured SOAP notes in seconds
- Place finalized notes into your EHR or practice management system
Lindy works in the background so you can focus on patient care. Instead of spending 10-15 minutes per visit writing notes, you review and finalize them in minutes while keeping full clinical control.
Try Lindy for free and reduce SOAP note time across your clinic.
FAQs
What is a SOAP note in physical therapy?
A SOAP note in physical therapy is a documentation format with four sections: Subjective (what the patient says), Objective (what you measure), Assessment (what it means), and Plan (what you did and what's next). This structure helps therapists document care, track progress, and justify treatment to insurance companies.
What is the SOAP note format?
The SOAP note format divides documentation into Subjective, Objective, Assessment, and Plan sections. Subjective captures what the patient tells you. Objective records what you measure and see. Assessment explains your clinical reasoning. Plan outlines treatment performed and future steps.
How detailed should physical therapy SOAP notes be?
Physical therapy SOAP notes should include enough detail to justify skilled treatment and track measurable progress. Record specific measurements (movement in degrees, strength grades, pain scales). List treatments with dosage. Explain your clinical reasoning. Avoid excessive detail—focus on information that supports medical necessity and shows change over time.
Are SOAP notes required for insurance and billing?
Yes, insurance companies require SOAP notes to verify that physical therapy services meet medical necessity rules. Your documentation must show skilled treatment, measurable progress toward functional goals, and appropriate treatment frequency. Incomplete or vague notes can result in claim denials or requests for more documentation.
Can SOAP notes be used across other therapies?
Yes, SOAP notes can be used across multiple healthcare fields, including occupational therapy, speech therapy, mental health counseling, chiropractic care, and massage therapy. The four-section format adapts to any field that requires systematic documentation of patient care and clinical reasoning.
References
- Chapman JS. Defining the profession through diagnostic reasoning. Physical Therapy. 1995;75(3):203. Available from: http://ptjournal.org/cgi/content/abstract/75/3/203
- O'Sullivan SB, Schmitz TJ, Fulk GD. Physical Rehabilitation. 6th ed. Philadelphia: F.A. Davis Company. Available from: https://hsrc.himmelfarb.gwu.edu/books/85/
- Podder V, Lew V, Ghassemzadeh S. SOAP Notes. In: StatPearls [Internet]. Bethesda: National Library of Medicine; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482263/













Blog
Related Articles

%20(1).png)
%20(1).png)

%2520(1).png)
The AI assistant that runs your work life
Lindy saves you two hours a day by proactively managing your inbox, meetings, and calendar, so you can focus on what actually matters.
